





Introduction
Workplace violence (WPV) refers to assaults associated with the workplace, resulting in physical and emotional harm to individuals and damage to resources.1 In recent years, violence against medical staff had been frighteningly common and attracted widespread attention.2 Healthcare workers, including doctors, nurses, and other medical staff, had a higher risk of experiencing WPV due to the nature of their work. Although the incidence of violence varied in each country, it was generally higher than 50%.3 According to data from the United States, WPV occurring in the medical environment accounted for almost 70.0% of all WPV incidents.4 Noticeably, among victims suffering WPV in healthcare settings, nurses are most often subjected to violent incidents due to long-term care and exposure to patients.5,6 The phenomenon of nurses suffering from WPV was more severe in developing countries with poor nursing conditions.7 Out of 1264 surveyed Bangladeshi nurses, 70% reported experiencing WPV. A total of 324 nurses reported experiencing physical violence, while 902 nurses reported experiencing non-physical violence.8 Besides, Zhang et al conducted a large-scale survey in 28 Chinese hospitals and discovered that the prevalence of WPV among 4125 nurses was 68.31%. Verbal abuse (61.25%) had been the most common form of violence, followed by threats (36.75%), physical violence (25.90%), and sexual harassment (2.76%).9 Edward et al (2016) reported the incidence of WPV among nurses in psychiatric department was three times higher than that of nurses in other departments. A systematic review by Li L et al indicated that the incidence of WPV among psychiatric nurses in China was 78%.10 In addition, a meta-analysis of nurses in healthcare settings showed the incidence of violence in psychiatric hospitals was higher than that in other medical units.11 Psychiatric patients were more likely to pose violence toward other people under the control of diseases, thus WPV was frequent in psychiatric hospital. The time of violent behavior was difficult to predict, and psychiatric nurses had the most contact with patients. Therefore, they would inevitably suffer a series of violent behaviors, including verbal abuse, threats, and even physical assaults. The occurrence of violence had caused great physical and psychological harm to nurses, leading to decrease of job satisfaction and work efficiency, and nursing quality. Empirical studies had shown that nurses who gone through WPV had a higher level of turnover intention,12 a higher risk of burnout (RR = 3.65, CI: 2.40–5.56)13 and were more prone to depression14 and mental disorders compared to those non-exposed to WPV. WPV had become an important issue that endangered the occupational safety of psychiatric nurses, inducing heavy psychological burden. Therefore, positive psychological intervention would be pressing.
With the rise of positive psychology, the new perspective of traumatic psychology research believed that setbacks, trauma and suffering contained the possibility of positive change. Tedeschi and Calhoun first proposed the concept of “post-traumatic growth (PTG)” in 1995, which referred to the tenacious struggle of individuals with traumatic events.15 Previous studies had shown that experiencing WPV could make the victim stressed.16 Although traumatic events might cause post-traumatic negative symptoms, the negative experience could be a “catalyst” for positive changes, a growing number of studies showed positive PTG resulting from coping with trauma.17,18
Empathy refers to an attempt to understand the pain of others.19 Jeffrey proposed dividing the concept of empathy into four dimensions: emotion, cognition, behavior, and morality.20 Empathy was a fundamental skill for healthcare workers.21 Research had shown that victims who experienced WPV might experience symptoms such as fatigue, decreased motivation, and poor workplace performance. Psychiatric nurses might decrease their empathy towards patients due to a lack of energy and emotion.22
Feeling confident in coping with patient aggression was crucial to provide nursing services smoothly for psychiatric nurses.23 Nurses who lacked confidence were unlikely to carry out nursing work smoothly. Previous studies had shown that individuals with confidence had higher levels of post-traumatic growth when facing traumatic events.24
Post-traumatic stress disorder (PTSD) refers to the individuals’ response to threatening events or environments. Individuals who experienced PTSD tended to recreate the scene and increase their alertness.25 Research showed that nurses who had suffered from WPV were 2–4 times more likely to suffer from PTSD compared to them who had never experienced.26 PTSD was not only related to external factors such as social acceptance and external concern, but also had an association to internal factors such as the patient’s own time perspective and psychological trends.27
Resilience refers to the ability of individuals to maintain mental health or resist negative emotions when facing trauma, stress, or difficulties.28 Hershner et al discovered that resilience could serve as a protective factor to dilute the negative effects of adverse psychological stress, which was beneficial for the growth of trauma and accelerated recovery of people.29
Recent studies had found that PTG made a difference to recovery of adverse mood after experiencing WPV.30 Studies had investigated risk factors of PTG in the past, such as introversion, job burnout and so on.31,32 However, limited studies explored the protective factors of PTG.32,33 Previous research had revealed that PTG were associated with resilience and self-confidence.24,34 A study reported that empathy, a psychological trait, could help individuals better cope with WPV and trigger more positive emotional experiences.35 Clarifying the level and protective factors of PTG aids in mental recovery of psychiatric nurses after experiencing WPV. For nursing managers, identifying the influencing factors of PTG could help recognize vulnerable nurses, intervene in vulnerable groups as soon as possible, and take targeted measures to reduce the impact of negative psychology.
This study aims to investigate the characteristics of PTG in psychiatric nurses who experienced violence in the workplace and analyze its influencing factors.
Methods
Study Design and Population
The study recruited 1202 psychiatric nurses from 5 tertiary hospitals in Guangdong from October 2022 to December 2022 using convenient sampling method. Inclusion criteria: 1) registered nurse; 2) had engaged in nursing work in the psychiatric department in recent 6 months; 3) had fundamental communication skills and agreed to sign informed consent; 4) had suffering from WPV including verbal abuse, physical violence, sexual harassment in the past six months. Exclusion criteria: 1) had been absent from position due to maternity and sick leave; 2) student nurses and nursing interns; 3) individuals with mental and psychological disorders; 3) poor compliance and inability to cooperate with questionnaire filling. Informed consent was obtained from all participants involved in the study.
Sample Size
Calculate the formula

The maximum number of dimensions in the scale used in this study was 5, and the maximum sample size calculated was 120. A total of 1202 subjects were included in this study, which met the sample size inclusion criteria.
Questionnaire Development and Data Collection Procedure
This study conducted a questionnaire survey by a online survey platform, and sent the QR code of the questionnaire to directors of nursing department or head nurses in 5 tertiary hospitals in Guangdong China. Then directors or head nurses forwarded the code to psychiatric nurses to fill out. The questionnaire adopted uniform guidelines to prevent possible bias, including the survey content, purpose, and filling requirements. The answer of each item was mandatory and one device could only fill in once. It ensured the completeness and accuracy of the questionnaire. The authors distributed and collected a total of 1216 questionnaires. Of the 1216 returned questionnaires, 1202 were complete, with an effective rate of 99.7%. This study excluded fourteen questionnaires due to logical issues, such as working years were greater than age. This study complied with the EQUATOR (STROBE) checklist.
Independent and Dependent Variables
The dependent variable of this study was the post-traumatic growth level of psychiatric nurses after experiencing WPV. The independent variables included general information of participants (gender, age, marital status, from single-child family, nursing experience, education background, professional title, employment form, ward type, hospital level and nature of hospital). In addition, empathy ability, the confidence in coping with WPV, post-traumatic stress disorder, and resilience of psychiatric nurses were also independent variables in this study.
Questionnaire
General Information
This study adopted a self-designed questionnaire to collect gender, age, marital status, from single-child family, nursing experience, education background, professional title, employment form, ward type, hospital level and nature of hospital.
Post-Traumatic Growth Inventory (PTGI)
Post-Traumatic Growth Inventory (PTGI), developed by Tedeschi and Calhoun, was an assessment tool for measuring PTG levels.36 The initial version included 21 items in 5 dimensions. The study adopted.a Chinese version with 20 items. The scale consisted of 5 dimensions, namely insights on life (6 items), personal strength (3 items), new possibilities (4 items), relationships with others (3 items), and self-transformation (4 items). The scale used the Likert 5 scoring system. Scores ranged from 0 to 100. Higher score suggested higher level of PTG. A total score >60 or average item score >3 indicated moderate and higher levels of PTG.37,38 In the study, Cronbach’s α was 0.978.
Jefferson Scale of Empathy Health Professional (JSE-HP)
Jefferson Scale of Empathy Health Professional (JSE-HP), compiled by Moha mmadreza Hoja et al,39 was an assessment tool for measuring the level of empathy among medical staff. The scale consisted of 20 items, including three dimensions: viewpoint selection (10 items), emotional care (8 items), and empathetic thinking (2 items). The dimensions of emotional care and empathetic thinking adopted the reverse scoring method. The scale used the Likert 7 scoring system, (1 = strongly disagree,7= strongly agree). Higher scores on the JSE-HPS indicated greater empathy, and scores could range from 20 to 140.40,41 In this study, Cronbach’s α was 0.913.
Confidence in Coping with Patient Aggression Instrument (CCPAI)
Confidence in Coping with Patient Aggression Instrument (CCPAI), developed by Thackrey in 1987, was an assessment tool for measuring the level of confidence in coping with patients’ aggressive behavior.42 The study selected the Likert 11 rating for 10 items, with each item scoring from 1 point (low confidence) to 11 points (high confidence). Scores ranged from 0 to 110. Higher score indicated higher level of confidence. The study by Xiurong Deng (2021) had found Cronbach’s α was 0.92, which had good reliability.23 In the study, Cronbach’s α was 0.964.
Post-Traumatic Stress Disorder Checklist-Civilian Version (PCL-C)
Post-traumatic Stress Disorder Checklist-Civilian Version (PCL-C) was developed by the PTSD Center in the United States in 1994. Yang Xiaoyun translated the scale into Chinese in 2007.43 Response options ranged from 1 (not at all) to 5 (seriously). The scale contained 17 items, and total scores ranged from 17 to 85. Researchers classified participants with a cutoff score of 38 or higher as having symptoms of post-traumatic stress disorder.44 In this study, the scale presented good internal consistency, and Cronbach’ s α of the PCL-C was 0.980.
Connor-Davidson Resilience Scale (CD-RISC)
Connor-Davidson Resilience Scale (CD-RISC), developed by Connor et al, consisted of 25 items to assess individuals’ level of psychological resilience. All items of the CD- RISC used a five-point response scale (0 = “not true at all” to 4 = “true nearly all the time”). The scores of respondents was based on how they had felt over the past one month and how much they agreed with each item. Total scores ranged from 0 to 100. Higher scores indicated higher resilience.45 In this study, Cronbach’ s α of the scale was 0.978.
Statistical Analysis
This study adopted SPSS 25.0 to process the data. Firstly, we conducted a descriptive analysis of general information on psychiatric nurses who suffered from WPV. We used t-tests or one-way ANOVA to compare the intergroup differences of demographic characteristics and scores of scales. Next, we studied the multicollinearity between independent variables. The results indicated that the VIF values were all below 10, indicating that there was no collinearity between the independent variables. Therefore, we used a multiple linear regression model to explore the factors influencing PTGI scores of psychiatric nurses after experiencing WPV. And the level of significance was set at 0.05.
The basic model is as follows:

β0 is a constant term. β1, β2, … βm are partial regression coefficients. X1,X2, … Xm are the independent variables.
Results
General Information of Participants
Among 1202 respondents, 236 were males (19.6%) and 966 were females (80.4%); Participants aged 21–30 accounted for the highest proportion (43.3%). The number of married psychiatric nurses far exceeded that of unmarried ones; The majority had a undergraduate’s degree in education (60.0%); In terms of working years, the proportion of nurses who had worked for ≤10 years was the highest, reaching 55.1% (Table 1).
 |
Table 1 General Information of Participants |
Total Score of PTGI and the Average Score of Items
The average PTGI score was 65.75 points, which was above the midpoint of the range. The average score of 20 items was 3.29 points. Examining each item, the highest score was “insights on life” with 26.66 points, followed by “self-transformation” (17.04), “new possibilities” (15.97), “personal strength” (13.20), and “relationship with others” (12.55) (Table 2).
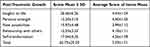 |
Table 2 Total Score of PTGI and the Average Score of Items Among Psychiatric Nurses in China 2023 |
Results of Bivariate Analysis of PTGI in Psychiatric Nurses
The results showed that the analysis results of marital status, from single-child family, education background, professional title, employment form, level of hospital, JSE-HP score, CCPAI score and CD-RISC score were statistically significant (P<0.05). (Tables 3 and 4)
 |
Table 3 The Relationship Between Demographic and PTGI Among Psychiatric Nurses in China 2023 |
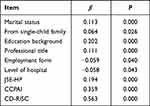 |
Table 4 Multivariate Linear Regression Analysis of PTGI Among Psychiatric Nurses in China 2023 |
Results of Linear Regression Analysis of PTGI in Psychiatric Nurses
The linear regression analysis model was established by taking the score of PTGI as the dependent variable, and the statistically significant variables of self-sample t-test and one-way ANOVA as independent variables. The results showed that from single-child family, education background, the confidence in coping with patient aggression, empathy and resilience were the main influencing factors of post-traumatic growth (P<0.05). Compared to from single-child family, psychiatric nurses who were non-single child had higher level of PTG (β=0.052, P=0.026). Psychiatric nurses who had master degree or above had higher level of PTG than those had certificate for occupation, diploma and bachelor degree (β=0.108, P<0.001). The stronger the empathy, the higher the level of PTG (β=0.057, P=0.024). The higher score of confidence in coping with patient aggression, the better PTG (β=0.106, P<0.001). Psychiatric nurses with good resilience had a higher level of PTG compared to nurses with poor resilience (β=0.484, P<0.001) Among all factors that affect the PTG of psychiatric nurses, resilience was the most influencing factor (β=0.484) (Table 5).
 |
Table 5 Variables Associated with PTGI Identified from Multiple Linear Regression Model Among Psychiatric Nurses in China 2023 |
Discussion
This study found that from single-child family, education background, the confidence in coping with patient aggression and resilience were protective factors for post-traumatic growth. The results of the study showed that total score of PTGI of psychiatric nurses was significantly higher than the PTGI score of clinical nurses in Lin Min’s study, (65.75±20.20±20.20) vs (57.16±21.53).46 The score indicated that psychiatric nurses had positive psychological changes after experiencing workplace violence. Empirical findings had found that violence in psychiatry department was relatively unpredictable And psychiatric nurses who had been exposed to frequent violent events for a long time had relatively strong ability to solve trauma events and internal resilience.47 After suffering from trauma, individuals would self-adjust to post-traumatic psychology and regard traumatic events as “rationalized events”, so that they could gradually accept post-traumatic changes.48 Among five dimensions of PTG, the score of insights on life dimension was the highest, which suggested that psychiatric nurses were aware of how to think and comprehend life and change their cognition after experiencing workplace violence. On the contrary, relationship with others dimension items had the lowest average score. Due to the occurrence of WPV, colleagues or others were unable to provide timely and effective assistance. In addition, the hospital’s reporting system for WPV was not perfect, so psychiatric nurses might feel disappointed. Therefore, nursing management personnel could improve the post-traumatic growth level of psychiatric nurses by guiding them to actively think things out for themselves from traumatic events, cultivate new interests and explore new possibilities.49
Previous studies had shown that both personal social and psychological factors had a certain impact on the post traumatic growth of psychiatric nurses.50 Among social factors, psychiatric nurses who were non-single child had higher level of post-traumatic growth. Due to social and cultural factors, individuals from single-child family were more likely to be lack of experience in living and emotionally communicating with their peers. Low level of interaction with siblings and excessive protection from family members resulted in varying degrees of differences in personality, value orientation, and other aspects. Therefore, single child had lower levels of post-traumatic growth. The higher the education background of psychiatric nurses, the higher their PTGI scores, which was consistent with the results of multiple studies conducted in different populations. The level of higher education could endow individuals with rich cognitive backgrounds, and individuals with higher educational backgrounds were more inclined to confide and communicate with others when encountering difficulties.51 Hence communication might be a protective factor for post-traumatic growth. For this reason, nursing managers should reasonably allocate human resources in the ward, optimize the structure of nurses, and encourage to communicate with each other through mutual communication so as to promote the transmission of positive psychological experiences.
Psychological factors also had significant impacts on post-traumatic growth of psychiatric nurses. Among them, the higher score of confidence in coping with patient aggression, the better post-traumatic growth. This might be in connection with the importance of confidence when dealing with attacks, which was a prerequisite for all treatment interactions.23 Besides, the study also suggested that the better the empathy ability of psychiatric nurses, the higher levels of post-traumatic growth among nurses. Nurses with strong empathy were able to empathize more with psychiatric patients, understand and experience feelings of patients. Thus, they had a greater understanding of workplace violence than nurses with low empathy. In addition, psychiatric nurses had higher scores of psychological resilience with higher scores of PTGI after WPV. The result might be related to people with higher psychological resilience who had stronger adaptability to severe stress situations for instance adversity, trauma, tragedy, and threats. Therefore, regular violence response training could be essential to help improve the confidence in coping with patient aggression of psychiatric nurses. As a result, hospital administrators and nursing managers should pay attention to psychiatric nurses with insufficient confidence, actively organize discussions and reflections on violent incidents. At the same time, the importance of resilience and empathy ability in the development of psychiatric nurses following violence should not be overlooked. Positive psychological intervention, mindfulness training,52 and other strategies could be useful to actively explore and raise the potential of psychiatric nurses’ resilience and empathy ability. Therefore, confidence in coping with patient aggression, empathy and psychological resilience were demanding.
Limitation in this study was that participants were from five tertiary hospitals in Guangdong, China, this might affect the generality of our findings, further large-sample investigation is needed.
Conclusion
This study explored the characteristics of PTG in psychiatric nurses who experienced violence in the workplace and analyze its influencing factors. The results showed that from single-child family, education background, the confidence in coping with patient aggression, empathy, and resilience were associated with PTG level. These insights are valuable for hospitals and nursing managers, providing a foundation for developing strategies, enabling them to identify vulnerable individuals and take early intervention measures against such populations. In addition, these findings emphasize the importance of PTG as a positive psychological factor, as it could improve the psychological level of psychiatric nurses in coping with WPV.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study obtained ethical approval from the IRB of the Affiliated Brain Hospital of Guangzhou Medical University (approval number: 2022-081). Informed written consent was obtained from all participants before inclusion. The entire study was carried out in accordance with the Declaration of Helsinki.
Consent for Publication
All patients in this study agree to publish.
Acknowledgments
We would like to thank all the participants who have contributed to this study.
Funding
This study is funded by Guangzhou Science and Technology Plan Project (grant number: 2023A03J0848).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Boafo IM. The effects of workplace respect and violence on nurses’ job satisfaction in Ghana: a cross-sectional survey. Hum Resour Health. 2018;16(1):6. doi:10.1186/s12960-018-0269-9
2. Seun-Fadipe CT, Akinsulore AA, Oginni OA. Workplace violence and risk for psychiatric morbidity among health workers in a tertiary health care setting in Nigeria: prevalence and correlates. Psychiatry Res. 2019;272:730–736. doi:10.1016/j.psychres.2018.12.177
3. Edward KL, Ousey K, Warelow P, et al. Nursing and aggression in the workplace: a systematic review. Br J Nurs. 2014;23(12):653–654, 656–659. doi:10.12968/bjon.2014.23.12.653
4. Rossi MF, Beccia F, Cittadini F, et al. Workplace violence against healthcare workers: an umbrella review of systematic reviews and meta-analyses. Public Health. 2023;221:50–59. doi:10.1016/j.puhe.2023.05.021
5. Johnsen GE, Morken T, Baste V, et al. Characteristics of aggressive incidents in emergency primary health care described by the Staff Observation Aggression Scale – Revised Emergency (SOAS-RE). BMC Health Serv Res. 2020;20(1):33. doi:10.1186/s12913-019-4856-9
6. Acquadro Maran D, Cortese CG, Pavanelli P, Fornero G, Gianino MM. Gender differences in reporting workplace violence: a qualitative analysis of administrative records of violent episodes experienced by healthcare workers in a large public Italian hospital. BMJ Open. 2019;9(11):e031546. doi:10.1136/bmjopen-2019-031546
7. Njaka S, Edeogu OC, Oko CC, Goni MD, Nkadi NL. Work place violence (WPV) against healthcare workers in Africa: a systematic review. Heliyon. 2020;6(9):e04800. doi:10.1016/j.heliyon.2020.e04800
8. Chowdhury SR, Kabir H, Das DC, Chowdhury MR, Chowdhury MR, Hossain A. Workplace violence against Bangladeshi registered nurses: a survey following a year of the COVID-19 pandemic. Int Nurs Rev. 2023;70(2):219–228. doi:10.1111/inr.12802
9. Zhang L, Wang A, Xie X, et al. Workplace violence against nurses: a cross-sectional study. Int J Nurs Stud. 2017;72:8–14. doi:10.1016/j.ijnurstu.2017.04.002
10. Li L, Zhang Q, Yang H, Undergraduate SL. Incidence and related influencing factors of workplace violence among psychiatric nurses in China: a systematic review and Meta-analysis. Arch Psychiatr Nurs. 2022;40:68–76. doi:10.1016/j.apnu.2022.04.005
11. Pariona-Cabrera P, Cavanagh J, Bartram T. Workplace violence against nurses in health care and the role of human resource management: a systematic review of the literature. J Adv Nurs. 2020;76(7):1581–1593. doi:10.1111/jan.14352
12. Kabir H, Chowdhury SR, Tonmon TT, et al. Workplace violence and turnover intention among the Bangladeshi female nurses after a year of pandemic: an exploratory cross-sectional study. PLOS Glob Public Health. 2022;2(4):e0000187. doi:10.1371/journal.pgph.0000187
13. Chowdhury SR, Kabir H, Chowdhury MR, Hossain A. Workplace bullying and violence on burnout among Bangladeshi registered nurses: a survey following a year of the COVID-19 pandemic. Int J Public Health. 2022;67:1604769. doi:10.3389/ijph.2022.1604769
14. Chowdhury SR, Kabir H, Mazumder S, Akter N, Chowdhury MR, Hossain A. Workplace violence, bullying, burnout, job satisfaction and their correlation with depression among Bangladeshi nurses: a cross-sectional survey during the COVID-19 pandemic. PLoS One. 2022;17(9):e0274965. doi:10.1371/journal.pone.0274965
15. Tedeschi RG, Calhoun LG. Trauma & transformation: growing in the aftermath of suffering. PsycCRITIQUES. 1995;42(2).
16. Pihl-Thingvad J, Andersen LL, Brandt LPA, Elklit A. Are frequency and severity of workplace violence etiologic factors of posttraumatic stress disorder? A 1-year prospective study of 1,763 social educators. J Occup Health Psychol. 2019;24(5):543–555. doi:10.1037/ocp0000148
17. Wu X, Kaminga AC, Dai W, et al. The prevalence of moderate-to-high posttraumatic growth: a systematic review and meta-analysis. J Affect Disord. 2019;243:408–415. doi:10.1016/j.jad.2018.09.023
18. Schubert CF, Schmidt U, Rosner R. Posttraumatic growth in populations with posttraumatic stress disorder-a systematic review on growth-related psychological constructs and biological variables. Clin Psychol Psychother. 2016;23(6):469–486. doi:10.1002/cpp.1985
19. Sinclair S, Beamer K, Hack TF, et al. Sympathy, empathy, and compassion: a grounded theory study of palliative care patients’ understandings, experiences, and preferences. Palliat Med. 2017;31(5):437–447. doi:10.1177/0269216316663499
20. Jeffrey D. Empathy, sympathy and compassion in healthcare: is there a problem? Is there a difference? Does it matter? J R Soc Med. 2016;109(12):446–452. doi:10.1177/0141076816680120
21. Winter R, Leanage N, Roberts N, Norman RI, Howick J. Experiences of empathy training in healthcare: a systematic review of qualitative studies. Patient Educ Couns. 2022;105(10):3017–3037. doi:10.1016/j.pec.2022.06.015
22. Nam SH, Lee DW, Seo HY, et al. Empathy with patients and post-traumatic stress response in verbally abused healthcare workers. Psychiatry Invest. 2021;18(8):770–778. doi:10.30773/pi.2021.0066
23. Deng XR, Xia ZC, Ye JR, Kuang SY. Investigation and analysis of psychiatric nurses’ confidence in coping with patient aggression. Nursing Prac Res. 2021;18(13):2026–2028. in Chinese.
24. Cui PP, Wang PP, Wang K, Ping Z, Wang P, Chen C. Post-traumatic growth and influencing factors among frontline nurses fighting against COVID-19. Occup Environ Med. 2021;78(2):129–135. doi:10.1136/oemed-2020-106540
25. Simon N, Robertson L, Lewis C, et al. Internet-based cognitive and behavioural therapies for post-traumatic stress disorder (PTSD) in adults. Cochrane Database Syst Rev. 2021;5(5):CD011710. doi:10.1002/14651858.CD011710.pub3
26. Havaei F. Does the type of exposure to workplace violence matter to nurses’ mental health? Healthcare. 2021;9(1):41. doi:10.3390/healthcare9010041
27. Hong D, Lin M, Zhang JY, Wu CL, Wu P, Meng J. Research progress of time perspective therapy and the enlightenment of time perspective therapy to nurse post-traumatic stress disorder in our country. Chin J. Pract Nurs. 2016;32(17):1356–1360.
28. Määttänen I, Henttonen P, Väliaho J, et al. Positive affect state is a good predictor of movement and stress: combining data from ESM/EMA, mobile HRV measurements and trait questionnaires. Heliyon. 2021;7(2):e06243. doi:10.1016/j.heliyon.2021.e06243
29. Hershner S, Auckley D. Perioperative management of insomnia, restless legs, narcolepsy, and parasomnias. Anesth Analg. 2021;132(5):1287–1295. doi:10.1213/ANE.0000000000005439
30. Zhang H, Dong L, Shang PP, Guan CY. Analysis of post-traumatic growth characteristics and influencing factors of psychiatric nurses who experienced violence in the workplace. J Neurosci Mental Health. 2021;21(5):356–360. in Chinese.
31. Zhang Y, Huang JB, Qiu DY. Influencing factors of posttraumatic growth among nurses suffering from workplace violence. Nurs J Chin People’s Liberat Army. 2018;35(12):17–21. in Chinese.
32. Fang YY, Qian RL, Wu T. Status quo and influencing factors of post traumatic growth of psychiatric nurses after adverse events. Chin Nurs Res. 2022;36(22):4106–4110. in Chinese.
33. Shen J. The impact of alexithymia on the growth of nurses who have been traumatized by workplace violence. Modern Nurse. 2019;26(7):27–30. in Chinese.
34. Han SJ, Chun JY, Bae HJ. Post-traumatic growth of nurses in COVID-19 designated hospitals in Korea. Int J Environ Res Public Health. 2022;20(1):56. doi:10.3390/ijerph20010056
35. Wang WC, Wu X. Mediating role of gratitude, social support and post-traumatic growth. Acta Psychologica Sinica. 2020;52(3):307–316. doi:10.3724/SP.J.1041.2020.00307
36. Tedeschi RG, Calhoun LG. The posttraumatic growth inventory: measuring the positive legacy of trauma. J Trauma Stress. 1996;9(3):455–471. doi:10.1002/jts.2490090305
37. Tang CS. Positive and negative postdisaster psychological adjustment among adult survivors of the Southeast Asian earthquake-tsunami. J Psychosom Res. 2006;61(5):699–705. doi:10.1016/j.jpsychores.2006.07.014
38. Wang Y, Xie H, Zhao X. Psychological morbidities and positive psychological outcomes in people with traumatic spinal cord injury in Mainland China. Spinal Cord. 2018;56(7):704–711. doi:10.1038/s41393-017-0044-0
39. An XQ, Yang H, Xu JP, Song LP, Qiu YF. CompiIation and evaluation of Jefferson empathic scaIe. Chin Nurs Res. 2008;22(22):2063–2064,2066. in Chinese.
40. Hojat M, Louis DZ, Maio V, Gonnella JS. Empathy and health care quality. Am J Med Qual. 2013;28(1):6–7. doi:10.1177/1062860612464731
41. Kiersma ME, Chen AM, Yehle KS, Plake KS. Validation of an empathy scale in pharmacy and nursing students. Am J Pharm Educ. 2013;77(5):94. doi:10.5688/ajpe77594
42. Thackrey M. Clinician confidence in coping with patient aggression: assessment and enhancement. Prof Psychol. 1987;18(1):57–60. doi:10.1037/0735-7028.18.1.57
43. Conybeare D, Behar E, Solomon A, Newman MG, Borkovec TD. The PTSD checklist-civilian version: reliability, validity, and factor structure in a nonclinical sample. J Clin Psychol. 2012;68(6):699–713. doi:10.1002/jclp.21845
44. Grubaugh AL, Elhai JD, Cusack KJ, Wells C, Frueh BC. Screening for PTSD in public-sector mental health settings: the diagnostic utility of the PTSD checklist. Depression Anxiety. 2010;24(2):124–129. doi:10.1002/da.20226
45. Connor RKM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18(2):76–82. doi:10.1002/da.10113
46. Lin M, Wang JL, He HJ, Li JW, Zhuang LL. Study on the current status and influencing factors of clinical nurses’ post-traumatic growth. Med Soc. 2020;33(7):82–85,109. in Chinese.
47. Chen Y. Analysis of the correlation between rumination level and post-traumatic growth status of emergency nurses suffering from workplace violence. J Nurs Train. 2021;36(2):150–153. in Chinese.
48. Peng W, Wang Q, Huang HX. Survey and analysis on the mental health of patients with maxillofacial trauma after comprehensive intervention. J Trauma Surg. 2011;13(6):529–531. in Chinese.
49. Li SR, Zhang XL, Zhang J. Emotional experience and coping strategies of psychiatric nurses after violence by patients. Chin Nurs Manag. 2017;17(3):297–300. in Chinese.
50. Oh JM, Kim Y, Kwak Y. Factors influencing posttraumatic growth in ovarian cancer survivors. Support Care Cancer. 2021;29(4):2037–2045. doi:10.1007/s00520-020-05704-6
51. Xu J, Liao Q. Prevalence and predictors of posttraumatic growth among adult survivors one year following 2008 Sichuan earthquake. J Affect Disord. 2011;133(1–2):274–280. doi:10.1016/j.jad.2011.03.034
52. Botha E, Gwin T, Purpora C. The effectiveness of mindfulness based programs in reducing stress experienced by nurses in adult hospital settings: a systematic review of quantitative evidence protocol. JBI Database System Rev Implement Rep. 2015;13(10):21–29. doi:10.11124/jbisrir-2015-2380
link
More Stories
Study shows that digital treatment with Tetris gameplay can dramatically reduce trauma memories
Emotional pain often outweighs fear in post-traumatic stress disorder
New Resource Empowers Trauma Survivors and Health Professionals