






Population characteristics
Six hundred fifty-three deaths of Salford residents occurred in weeks 12–19 of 2020: 106 died out of area, 4 deaths remained unregistered at the time of the evaluation, 19 had incomplete case records, and 2 could not be accessed in full. There were 522 cases which formed the final review cohort (Fig. 1). The characteristics of these 522 patients are found in Table 2. 51% were female, 35% had dementia, 81% were Caucasian, 9% of mixed or multiple ethnic origin, 10% for other ethnic minority backgrounds, age 79 ± 9 years, 64% cardiovascular co-morbidities. One hundred ninety-seven patients (38%) died in hospital, 190 (37%) in a care home, 120 (21%) at home, and the majority of the remainder in a hospice. Of hospital deaths, 13 died in the Emergency Department (ED) including 5 dead on arrival. Twenty-eight died in a critical care or respiratory high care area.
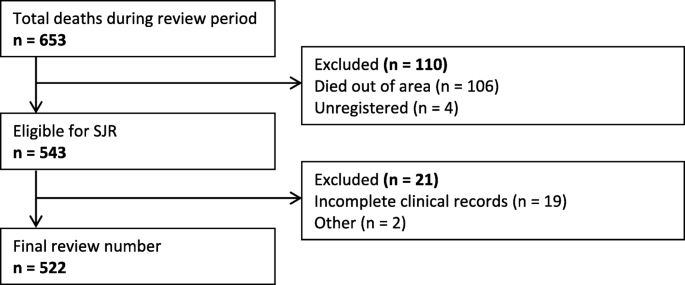
Review exclusion flowchart
Healthcare contact prior to death was most frequently with primary care (81% of patients). Forty-six patients (9%) had healthcare appointments cancelled (median 1 cancellation, range 1–9). There were 60 cases where delays in accessing care occurred.
The directive to prioritise use of the NHS 111 service had unintended adverse consequences. Fewer than half of NHS 111 calls were answered during this period. Twenty-seven of these (46%) resulted in advice to seek further care from their GP or in the community. 9 (15%) resulted in a delay in receiving this care, 5 of whom were seen later in the day by other services and subsequently admitted to hospital.
23% of patients were tested for COVID-19 (n = 203). 63% were positive (25% of the review population). The likelihood of a positive swab differed between location of death (68% in care homes, 20% in hospital, 30% in own home). COVID-19 was the most commonly listed cause of death. Eighty-seven of these (43%) did not have a positive swab result. Of the 286 who did not have COVID-19 on the death certificate, 80 (28%) had symptoms consistent with the diagnosis.
Avoidability of death scoring
80% of cases had an avoidability of death score of 6 allocated by the panel (definitely not avoidable). 18% had a score consistent with some degree of avoidability. 15% had a score of 5 or 4 (slight or possible avoidability). 3% of cases a score of 3 or 2 (more than 50:50 likelihood of being avoidable). None scored 1 (definitely avoidable). 2%, although reviewed for themes, had no final score allocated as these were sudden deaths in a patient’s home with no further information available: the panel did not feel scoring was possible.
The inter-observer agreement of individual reviewer scores was 79%. The free-marginal kappa was 0.75 (95% confidence 0.69–0.80). The fixed marginal kappa was 0.27 (0.12–0.42). Within the context of place of death, the number of cases with at least some potential avoidability were 30% for care home, 23% for death in own home, and 43% for death in hospital. For the age groups < 55 years, 55–75 years, > 75 years the respective figures were 40, 34, and 32%. In older patients, deaths in care homes scored < 6 less frequently than death in other locations (29% versus 53%). This indicates that older patients who resided in their own home were at greater risk of avoidable death than those residing in a care home. For Caucasian patients and non-Caucasian patients the respective figures were 19 and 16%. For COVID-19 and non-COVID-19 deaths the figures were 49 and 23%. The highest frequency of potential avoidability was in patients with learning disabilities (LD), albeit in a small number of deaths (4 of 9 deaths, Fig. 2).

Comparison of distribution of avoidability scores 2 to 5 (indicating findings consistent with some avoidability) between patient groups
Of the 16 scores of 2 or 3, there were 38 individual examples of recurring themes identified. These were most frequently: delay in accessing care (n = 11), below optimal care (n = 10), and language barriers (n = 3). There was also potentially avoidable COVID-19 contact, delayed response, misdiagnosis, and refusal to attend ED (Table 3).
There was a similar distribution in scores of 4 or 5 (also Table 3) with below optimal care, delays in testing, and delays in accessing care being most common. Themes which occurred relatively more frequently in these cases compared to scores of 2 or 3 were potentially avoidable COVID-19 contact (n = 19 of 154 cases) and delayed response (n = 15).
Deaths where more than one theme was identified were more common in cases with a greater likelihood of avoidability of death. For scores of 2 or 3, 44% of cases had more than 2 themes. For scores of 4 to 5, 35% of cases had more than 2, and for scores of 6, 17% of cases had more than 2.
Thematic review
An overview of the 53 patients (9%) showed a delayed presentation to medical services. Within General Practice there were 9 cases of below optimal care, 2 delayed response by clinicians, and 4 examples of lack of service capacity.
For deaths in hospital, there were 255 occasions of themes identified, affecting 129 patients. These included below optimal care in 79 patients, delay in testing 37 patients. Themes most often occurred prior to admission (69% delays in testing, 67% below optimal care, 29 of 30 delays in access). There were 9 hospital deaths after delayed presentation due to patient self-isolation. Four occasions of below optimal care in secondary care were found in patients who were allocated an avoidability score of 2 or 3. These were examples of absence of escalation to higher levels of care.
Residents in care homes were not sufficiently protected from COVID, and isolation from potential contacts with COVID may not have been fully enforced (Table 4). In cases of below optimal care, the majority were issues with Do Not Attempt CPR (uDNAR) directives and Advanced Care (ACP) or Gold Standard Framework (GSF) planning. This is within the broader context of generally excellent end of life planning (92% ACP, 97% uDNAR, and 69% GSF in place at the time of death). There were examples where ambulances were called despite all these being in place.
Two hundred ninety-four patients had called 999 (56%). The main theme was delay in response (20 cases). Eleven of these were in patients whose death was considered definitely not avoidable. Fifty-nine were recorded as having called NHS 111 (11%). There were 9 delays in care as a result of 111 calls (15% of calls). Details of the outcomes of all 111 calls and associated themes are found in Table 5. Significant delays in 999 response to Category 1 and 2 calls occurred contributing to avoidable factors in 9 deaths (3%) involving ambulance conveyance, significant delay being a response over three times the 90th Centile (Category 2 90th centile 40 min). The ambulance response took over 2 hours in 44% of Category 2 (immediate and life threatening) cases in March 2020 (mean time 126 min, maximum wait 328 min). The national ambulance response protocol was amended from 2nd April 2020 to mitigate against the emerging pandemic associated delays. This led to a reduction in category 2 delays as detailed in Table 5. Alongside this, the category 1 numbers may contain a number of category 2 ‘upgrades’ i.e. where a response was delayed until the call became critical and then upgraded. This is likely to explain the long dispatch time noted in some category 1 responses. However, it was not possible to differentiate clearly these upgraded calls within the available data. From the beginning of April 2020 no Category 2 patient waited longer than 96 min (mean 44 min, maximum wait 96 min, Table 6).
For ambulance conveyance to hospital with time from call to arrival < 2 h, 78% of patients had a NEWS2 ≥ 5 on arrival of the paramedic crew to the patient (mean score 7.1 ± 4.0). This compared with 68% for call to arrival 2–4 h (6.3 ± 3.3), and 48% for arrivals > 4 h (4.9 ± 3.6).
An overall summary of the key thematic findings is found in Table 7.
link
More Stories
Myanmar: Junta Assault on Health Care Hinders Quake Response
Crisis and Emergency Response | United Nations
Mission, B.C., residents demand urgent action amid persistent ER closures