






Sociodemographic characteristics of participants
The study included 180 women with FGM aged 18–53 years (mean age: 30.7 ± 7.2). The majority underwent FGM between ages 7–11 (57.8%, n = 104), while 30.6% (n = 55) and 11.7% (n = 21) experienced it during early childhood (6 months–6 years) or adolescence (12–22 years), respectively. Marital duration varied, with 33.9% (n = 61) married for 0–5 years. Nearly half (44.9%, n = 81) had four or more children. The educational attainment of participants varied, with 26.1% (n = 47) completing primary school, 18.3% (n = 33) middle school, and 22.8% (n = 41) higher education. The majority (77.2%, n = 139) resided in urban areas, and 72.8% (n = 131) identified as housewives (Table 1).
Perspectives on female genital mutilation
Participants cited various socio-cultural and religious justifications for undergoing FGM, with the most common being religious obligation (31.1%, n = 56), followed by tradition and customs (20.0%, n = 36), social pressure (13.8%, n = 25), preservation of virginity (11.1%, n = 20), and control over sexual desire (10.0%, n = 18), and 4.4% (n = 8) associated the practice with social acceptance (Table 2).
Emotional responses to female genital mutilation
On the day of the procedure, 58.9% (n = 106) of respondents reported feelings of “extreme fear and trauma,” while 17.8% (n = 32) reported feelings of “happiness and joy.” During the procedure itself, 60.6% (n = 109) described experiencing “fear, panic, and severe pain” (Table 2).
Physical consequences of female genital mutilation
The data demonstrate that long-term physical complications are prevalent, with 43.9% (n = 79) of participants reporting persistent health sequelae. Childbirth-related complications were the most frequently cited (47.8%, n = 86), followed by dysmenorrhea (47.8%, n = 86) and menorrhagia (33.3%, n = 60). Furthermore, 41.7% (n = 75) of the participants reported sexual dysfunction, including dyspareunia and reduced sexual desire, while 31.7% (n = 57) experienced chronic pelvic pain. The analysis also revealed additional morbidities, including vulvar pruritus (21.1%, n = 38), recurrent genitourinary infections (43.3%, n = 78), dysuria (37.8%, n = 68), impaired fertility (22.8%, n = 41), and structural genital abnormalities (18.9%, n = 34).
Views on the continuation of FGM
The findings of the study indicated that 43.8% of the participants reported satisfaction with undergoing FGM, while 55.9% expressed dissatisfaction. In terms of terminology preference, 42.2% of the participants favored positive descriptors for FGM, whereas 56.7% preferred negative words. Regarding the continuation of the practice, 38.3% of the participants supported its perpetuation, while 56.1% advocated for its cessation. An additional 4.4% of participants did not offer a opinion on the subject (Table 2).
FGM implementation and decision-making
Mothers were the primary decision-makers for FGM (71.7%, n = 129), followed by grandmothers (17.2%, n = 31); fathers, grandfathers, or aunts constituted 9.4% (n = 17). Most participants (56.7%, n = 102) underwent FGM unanticipatedly without prior explanation, while 15.0% (n = 27) experienced unanticipated procedures with explanation. Anticipated procedures occurred with explanation (17.2%, n = 31) or without (10.6%, n = 19). (Table 2).
PTSD symptoms exhibited significant positive correlations with all Brief Symptom Inventory (BSI) dimensions (r = 0.23–0.37, p < 0.01) and a negative association with resilience (r = − 0.27, p < 0.01). BSI subscales demonstrated strong intercorrelations, including somatization with obsessive–compulsive symptoms (r = 0.67, p < 0.01) and depression with anxiety (r = 0.69–0.70, p < 0.01).
Bidirectional relationships between PTSD and psychological symptoms were assessed via multiple linear regression. Predictors (sociodemographics, childhood trauma subtypes, resilience) were modeled bidirectionally: PTSD symptoms as the dependent variable with psychological symptoms as predictors, and vice versa. All predictors (nominal, ordinal, continuous) were entered simultaneously using stepwise selection, following confirmation of regression assumptions (VIF < 10, tolerance > 0.20). The PTSD symptom model explained 23.6% of variance (R2 = 0.236, F(4,122) = 10.74, p < 0.001), with dysmenorrhea (β = 0.22, t = 2.57, p < 0.05) and traumatic life experiences (β = 0.26, t = 3.20, p < 0.001) identified as significant positive predictors of PTSD symptoms. Resilience inversely predicted PTSD severity (β = − 0.19, p < 0.05). Interpersonal sensitivity (BSI-IS; β = 0.17, t = 2.11, p < 0.05) also contributed positively to PTSD severity.
In the first model, it was significant the direct effect of PTSD, which is the independent variable, on BRS (a1) (B = − 0.24, SE = 0.06, t = − 3.68, p < 0.001 and 95% CI [− 0.39 to − 0.11]) and of direct effect on CTQ-EN (a2) (B = − 0.06, SE = 0.03, t = − 2.13, p < 0.001 and 95% CI [− 0.12 to − 0.01]). In addition, obsessive compulsive symptoms, which is the dependent variable of the model, has a direct effect on BRS (b1) (B = − 0.08, SE = 0.04, t = − 2.18, p < 0.001 and 95% CI [− 0.15 to − 0.01]), and of direct effect on CTQ-EN (b2) (B = − 0.23, SH = 0.08, t = − 2.72, p < 0.001 and 95% CI [− 0.39 to − 0.06]). They were found to be significant the total effect on depression of PTSD (c) (B = 0.17, SE = 0.03, t = 5.29, p < 0.001 and 95% CI [0.11–0.23]) and direct effect (c’) (B = 0.14, SE = 0.03, t = 4.19, p < 0.001 and 95% CI [0.07–0.20]). The bootstrap method was used to test whether the effect of the mediator variable was significant, and since the confidence intervals did not include zero, the total indirect effect on obsessive compulsive symptoms was found to be significant (B = 0.03, SE = 0.01 and 95% CI [0.01–0.06]) (Fig. 1). Additionally, the model was found to be significant, explaining 14% of the variance (F(1,178) = 27.98, p < 0.05).
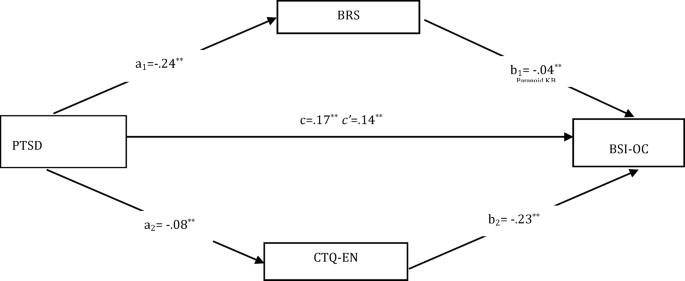
Parallel mediation effect of resilience and CTQ-EN in the relationship between PTSD and obsessive–compulsive symptoms PTSD: National Stressful Events Survey for post-traumatic stress disorder, CTQ-EN: Childhood Trauma Questionnaire- Emotional Neglect, BRS: Brief Resilience Scale, BSI-O-C: BSI (Brief Symptom Inventory)- Obsession–Compulsion.
In the second model, it was significant the direct effect of PTSD, which is the independent variable, on BRS (a1) (B = − 0.24, SE = 0.06, t = − 3.68, p < 0.001 and 95% CI [− 0.39 to − 0.11]) and of direct effect on CTQ-EN (a2) (B = − 0.06, SE = 0.03, t = − 2.13, p < 0.001 and 95% CI [− 0.12 to − 0.01]). In addition, depression, which is the dependent variable of the model, has a direct effect on BRS (b1) (B = − 0.04, SE = 0.03, t = − 1.29, p < 0.001 and 95% CI [− 0.10 to − 0.00]), and of direct effect on CTQ-EN (b2) (B = − 0.31, SH = 0.07, t = − 4.51, p < 0.001 and 95% CI [− 0.45 to − 0.17]). They were found to be significant the total effect on depression of PTSD (c) (B = 0.09, SE = 0.03, t = 3.40, p < 0.001 and 95% CI [0.04–0.15]) and direct effect (c’) (B = 0.06, SE = 0.03, t = 2.39, p < 0.001 and 95% CI [0.01–0.12]). The bootstrap method was used to test whether the effect of the mediator variable was significant, and since the confidence intervals did not include zero, the total indirect effect on depression was found to be significant (B = 0.03, SE = 0.01 and 95% CI [0.01–0.05]) (Fig. 2). Additionally, the model was found to be significant, explaining 6% of the variance (F(1,178) = 11.54, p < 0.05).
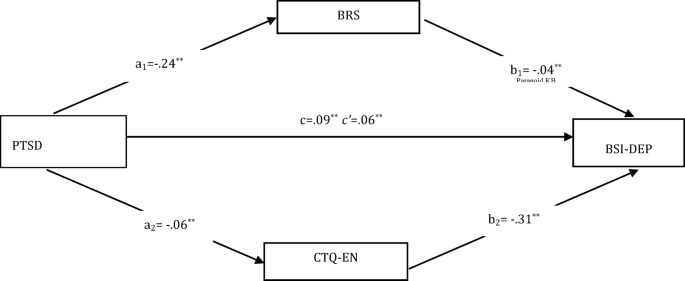
Parallel mediation effect of resilience and CTQ-EN in the relationship between PTSD and depression. PTSD: National Stressful Events Survey for post-traumatic stress disorder, CTQ-EN: Childhood Trauma Questionnaire- Emotional Neglect, BRS: Brief Resilience Scale, BSI-DEP: BSI (Brief Symptom Inventory)- Depression.
In the third model, it was significant the direct effect of PTSD, which is the independent variable, on BRS (a1) (B = − 0.24, SE = 0.06, t = − 3.68, p < 0.001 and 95% CI [− 0.39 to − 0.11]) and of direct effect on CTQ-EN (a2) (B = − 0.06, SE = 0.03, t = − 2.13, p < 0.001 and 95% CI [− 0.12 to − 0.01]). In addition, anxiety, which is the dependent variable of the model, has a direct effect on BRS (b1) (B = − 0.04, SE = 0.03, t = − 1.23, p < 0.001 and 95% CI [− 0.10 to − 0.00]), and of direct effect on CTQ-EN (b2) (B = − 0.18, SH = 0.07, t = − 2.55, p < 0.001 and 95% CI [− 0.33 to − 0.04]). They were found to be significant the total effect on anxiety of PTSD (c) (B = 0.10, SE = 0.03, t = 3.53, p < 0.001 and 95% CI [0.04–0.15]) and direct effect (c’) (B = 0.08, SE = 0.03, t = 2.69, p < 0.001 and 95% CI [0.02–0.13]). The bootstrap method was used to test whether the effect of the mediator variable was significant, and since the confidence intervals did not include zero, the total indirect effect on aggression was found to be significant (B = 0.02, SE = 0.01 and 95% CI [0.00–0.04]) (Fig. 3). Additionally, the model was found to be significant, explaining 7% of the variance (F(1,178) = 12.47, p < 0.05).
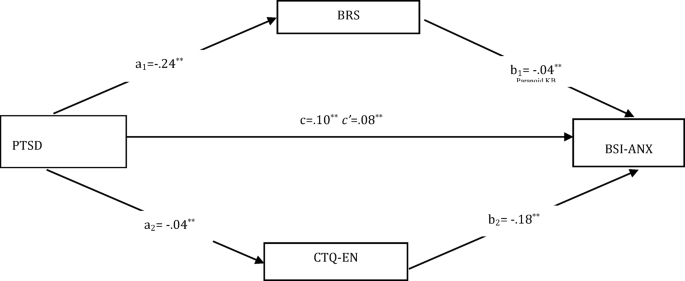
Parallel mediation effect of resilience and CTQ-EN in the relationship between PTSD and anxiety. PTSD: National Stressful Events Survey for post-traumatic stress disorder, CTQ-EN: Childhood Trauma Questionnaire- Emotional Neglect, BRS: Brief Resilience Scale, BSI-ANX: BSI (Brief Symptom Inventory)- Anxiety.
link
More Stories
Study shows that digital treatment with Tetris gameplay can dramatically reduce trauma memories
Emotional pain often outweighs fear in post-traumatic stress disorder
New Resource Empowers Trauma Survivors and Health Professionals