






Study design
The study employed descriptive cross-sectional design. This design collected data from healthcare workers at a single point in time to provide a snapshot of their current fire safety knowledge and preparedness levels at all three hospitals selected for the study [14]. The cross-sectional design enabled the description of the characteristics of a population and analyze relationships between the independent variables (socio-demographic characteristics) and the dependent variables (knowledge of emergency preparedness and fire safety) [15]. Cross-sectional studies are cost-effective and quick to conduct, and as such the researchers adopted this design because the study was not funded and was time bound.
The study is reported using Strengthening the Reporting of OBservational Studies in Epidemiology (STROBE) guideline (Supplementary file 1).
Study area
The study was conducted in the Kunene region of Namibia, encompassing the district hospital environments of Opuwo, Outjo, and Khorixas. Opuwo Hospital is located in north-western Namibia (Opuwo town) and, is the administrative capital of the Kunene Region, Khorixas District Hospital is positioned to the southwest of Opuwo and south of Outjo in Khorixas town while Outjo District Hospital is located in the town of Outjo, which is situated in the southern part of the Kunene Region in Namibia. All these three district hospitals act as referral centers for smaller clinics in the surrounding areas. Outjo and Khorixas district hospitals are in more accessible locations than Opuwo. Opuwo District Hospital being located in a remote area made it challenging in logistical issues such as delivery of supplies. Figure 1 shows the map of Namibia.

Study population and sample size
The target population of this study was all healthcare workers at all three hospitals in the region including student healthcare workers at all three hospitals. The sample size was determined based on the total number of healthcare workers available at each hospital during the study period by using mean and Standard deviation from preliminary results calculated using this formula:
$$n= ((Z\_(1-\alpha /2) \times \sigma )/\delta m )^{\wedge}2 \text{where}\,{\varvec{n}}=\text{ Sample size}, {\varvec{Z}}\,1-\boldsymbol{\alpha }/2= \mathrm{significant \,level \,of}\, 0.05 (95\% CI),{\varvec{\sigma}}= \text{Standard deviation},{\varvec{\delta}}= \text{Margin}/\text{ allowable error}.$$
Total population: Opuwo District Hospital = 170 HCWs
Outjo District Hospital = 114 HCWS
Khorixas District Hospital = 143 HCWs
Total = 427
Mean and Standard deviation from preliminary results
$$\overline{x }=4.875 \sigma = 3.72$$
$$n= ( (1.96 \times 3.73 )/0.5)^{\wedge}2=214\times 1.2 =256.8 \approx 257$$
Number of survey personnel per hospital were selected proportionately
Opuwo District Hospital = 102
Outjo District Hospital = 69
Khorixas District Hospital = 86
Figure 2 shows the selection process for the study participants.
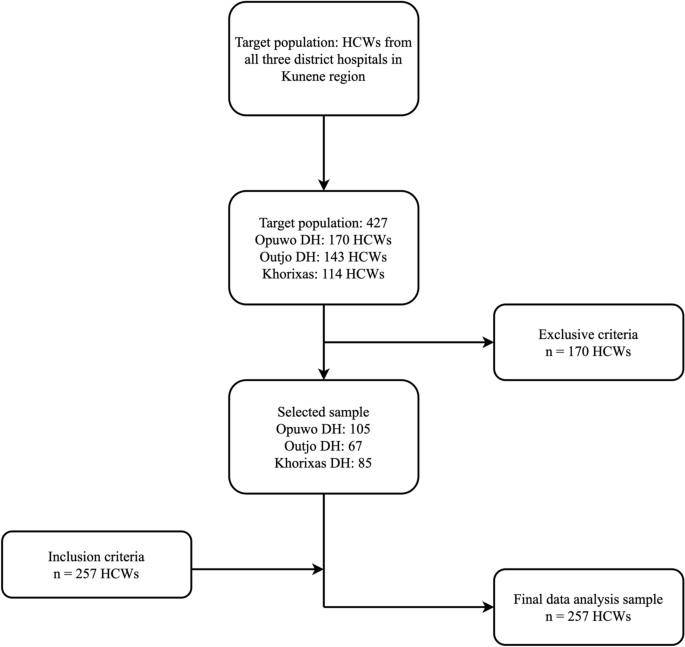
Flow chart of selection of participants
Data collection
A semi-structured questionnaire, adapted from the previous studies [16, 17], was used to collect data from the study participants. The questionnaire consisted of six sections. Section 1 of the questionnaire consisted of the Research title and introduction part of the researcher, Sect. 2 had the respondent’s consent part, Sect. 3 consisted of the demographic information of respondents, Sect. 4 with fire safety knowledge questions, Sect. 5 with emergency preparedness questions, and Sect. 6 for the conclusion. The questionnaire was built into an electronic questionnaire using google form. The link to the form was shared with the participants to complete. The researchers assigned co-researchers at all three district hospitals to collect data from participants who could not access the survey link.
The validity and reliability of the knowledge questions were assessed using Cronbach’s Alpha. Cronbach’s Alpha between 0.7 – 0.79 and 0.8 – 0.9 were considered acceptable and good, respectively [18]. The Cronbach’s alpha for fire safety and emergency preparedness knowledge was 0.73 and 0.87, respectively.
Sampling techniques
Participants were recruited using a stratified random sampling method. This approach involved dividing the healthcare workers into distinct strata based on their departments and job roles. Within each stratum, participants were randomly selected to ensure a representative sample from each category.
Healthcare workers were approached during their shifts and invited to participate voluntarily by the assigned co-researcher at all three health facilities. This method ensured that the sample included a diverse range of healthcare professionals, providing a comprehensive overview of the workforce.
Ethical consideration
The respondents were given an option of consent to participate in the study in the first section of the questionnaire, and they were assured that there would be no harm if they chose not to participate. Additionally, the researcher informed the participants that the data from the study would be used solely for educational research purposes and would be kept confidential. Respondents were treated fairly, especially during the selection process of the study sample, as each respondent had an equal chance of participating. The researcher also provided contact details in case the respondents needed clarification. To ensure validity and reliability, the researcher ensured that the instrument accurately represented all of the components of the study’s aims and objectives.
Data analysis and statistical techniques
The data were manually cleaned, and uploaded in the SPSS version 25.0 for coding and checking for discrepancies. The data was exported into STATA version 18 for analysis. Descriptive analysis, in the form of frequencies and percentages, was used to summarize the socio-demographic characteristics of the participants, as well as the variability of responses related to fire safety knowledge and emergency preparedness. Also, the level of knowledge of fire safety and emergency preparedness was summarized using descriptive statistics.
The fire safety knowledge section had 8 questions while emergency preparedness section had 9 questions, and Sect. 5 contained 9 questions. Both sections had three possible responses: ‘Yes’, ‘No’, and ‘Not sure’. ‘Yes’ marked a right answer, whilst ‘No’ and ‘Not sure’ represented incorrect answers. The questions and knowledge scores scales were adapted from the previous studies [17, 19]. Table 1 presents the score interpretation.
Pearson’s correlation analysis was also used to assess whether there were any correlations between fire safety and emergency preparedness parameters among healthcare workers. Additionally, logistic regression analysis was used to identify factors/ predictors that significantly influence the level of knowledge of fire safety and emergency preparedness among healthcare workers, at a significant level of p-value ≤ 0.05 at 95% confidence interval (CI).
Missing data
The study had a 100% response rate. Also, data cleaning was done to remove all inconsistencies and discrepancies in the data. The study had no missing data in the study.
link
More Stories
Myanmar: Junta Assault on Health Care Hinders Quake Response
Crisis and Emergency Response | United Nations
Mission, B.C., residents demand urgent action amid persistent ER closures